Thank you for choosing us as your eye doctor. Our goal is to build a strong partnership between you and our practice. To help ensure we can provide excellent service, please read our financial policy carefully. You should also know that we require you to pay for services before they begin. In addition, we require you to inform us of any changes in your personal information.
If your insurance company requests a referral and/or authorization, we will do our very best to get it for you. Ultimately you are responsible for ensuring that the referral and/ or authorization is received. Failure to receive it may result in a significant reduction in your compensation, and the remaining balance would be your responsibility.
The patient is expected at each visit to present a current health insurance card. All co-pay payments and prior balances are due upon arrival, unless previous arrangements have already been made with a billing representative. We accept cash, checks, Visa, MasterCard and Discover. Co-insurance/deductibles will be collected at time services are rendered. Should your previous balance not be paid or previous arrangements not be discussed with the billing department the examination, testing or procedure may be rescheduled/canceled.
INSURANCE CLAIMS
We will bill your insurance company and secondary insurance company as a courtesy to you, so that they know about your coverage. In order to properly charge your insurance companies, we require that you tell us everything about your insurance policies, including primary and secondary coverage, as well as any changes to your insurance policy. Failure to provide complete information may result in you paying the full amount of the bill. Although we can predict how much your insurance company will cover, the insurance company makes final decisions regarding your eligibility and benefits. If we are out-of-network for your insurance company and you receive direct payments, you are responsible for paying the balance.
SELF-PAY ACCOUNTS
Self-pay accounts refers to:
- Patients without insurance coverage
- Patients without insurance coverage who pay out of pocket
- Patients without an insurance card
- Patient without insurance coverage on file with us
- Patients without an insurance card who are uninsured
We do not accept attorney letters nor contingency fees.
It is always your obligation to know if our office is participating in your health plan. If there is any discrepancy in our information, then we will always consider a person self-pay unless proven differently. Self-pay patients must pay for services rendered at the initial visit. If you have extenuating circumstances, please contact our billing department to discuss a mutually agreeable plan. It is never intended to cause hardship to our clients. We only seek to offer the best care possible with minimal stress.
MEDICAL RECORDS
Patients, attorneys and insurance companies requesting copies of medical records will be charged as following, in accordance with Indiana State Law.
$20 labor fee
$1 per page (pages 1 through 10, only if no labor fee charged)
$0.50 per page (pages 11through 50)
$0.25 per page (pages 51 and higher)
Actual mailing costs (does not include “handling”)
$10 rush fee if records are to be provided within two business days
$20 certifying fee (if appropriate)
As always, if a collaborating physician (primary care, specialist or optometrist) requests portions of your record to assist in your care, there will be no charge.
OUTSTANDING BALANCE POLICY
Our office sends three statements to any patient with a past-due account. If payment is not made on your account, we will make one phone call and send one letter. If no resolution can be made, the account will be sent to the collection agency or attorney, and the patient will be discharged from the practice. In the event an account is turned over for collections, the person financially responsible for the account will be responsible for all collections costs, including third party costs, attorney fees and court costs.
Regardless of any personal arrangements that a patient might have outside of our office, if you are over 18 years of age and receiving treatment, you are ultimately responsible for payment of your services. Our office will not bill any other personal party.
This financial policy helps the office provide quality care to our valued patients. If you have any questions or need clarification of any of the above policies, please feel free to contact us.
The charge for a return check is $25, paid by cash or money order (not credit card). This will be added to your account balance in place of the insufficient funds amount. A returned check can only be used once. After that, we’ll apply the fee to your account balance.
The parent(s) or guardian(s) is responsible for full payment. Payment must be made prior to treatment of the minor. A signed Release to Treat Form may also be required for unaccompanied minors.

Specialty refractive surgery involves the use of advanced intraocular lenses (IOLs) to correct common vision problems during cataract surgery
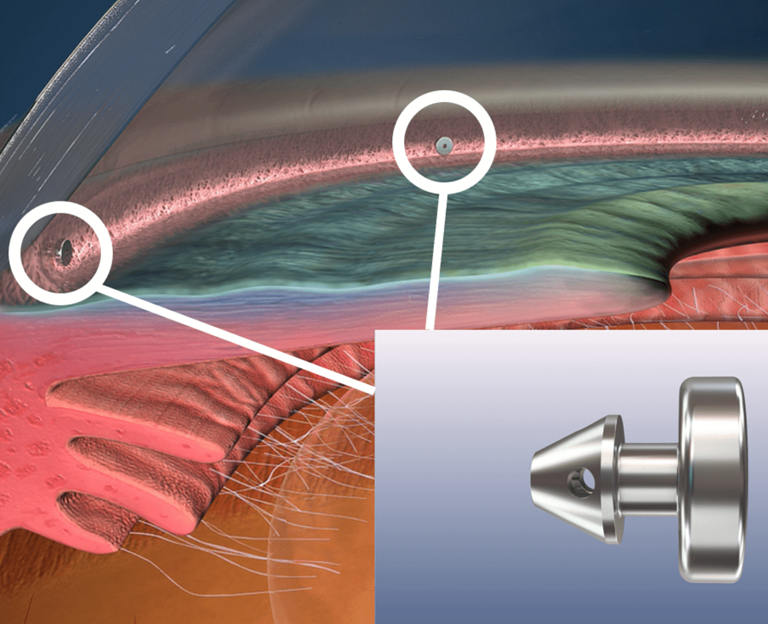
Minimally Invasive Glaucoma Surgery (MIGS) is a newer class of procedures designed to lower eye pressure
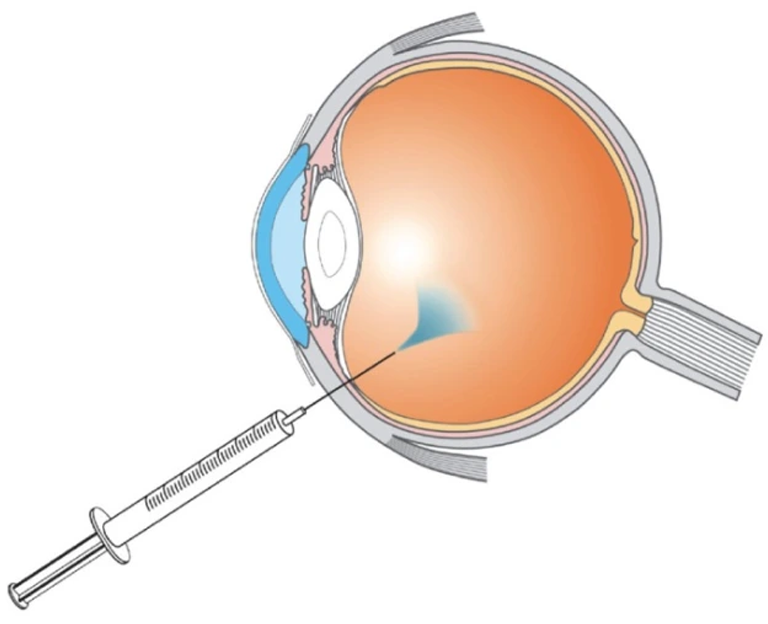
Intraocular injections are a highly effective treatment for a variety of retinal conditions.